Lichen sclerosus is an inflammatory skin condition. In women, it most commonly affects the skin around the vulva and the perianal area (the front and back passage).
Less often, it may appear on other parts of the body, including the thighs, under the breasts, the neck, shoulders and wrists.
What are the symptoms?
Lichen sclerosus often causes intense itching, irritation, and soreness of the vulval skin. These symptoms can lead to difficulties with passing urine or opening the bowels, and can make sex painful and difficult.
The skin may appear red and inflamed, but it can also look white, thickened, or scarred. It may also develop tiny purple blood blisters, and in some cases the skin can become raw.
Who is affected by Lichen sclerosus?
Lichen sclerosus usually affects adult women, but it can also affect children and men to a lesser extent. It is most commonly seen in women in their forties and fifties.
What causes Lichen sclerosus?
It is not known for certain what causes Lichen sclerosus. However, it is thought to be an autoimmune skin condition in which the body produces antibodies that may react against the skin of the vulva. It may also be associated with other autoimmune conditions, such as thyroid disease and diabetes.
Lichen sclerosus is not caused by an infection, it is not contagious, and it cannot be passed on to a sexual partner through contact.
Lichen sclerosus is not caused by the menopause, hysterectomy, the oral contraceptive pill or hormone replacement therapy (HRT). HRT or oestrogen creams do not treat the condition, although they may help with some symptoms.
Friction or rubbing of the skin can make the condition worse (the Koebner response). Exposure to urine may also increase irritation.
Lichen sclerosus may sometimes occur in other family members.
Can Lichen sclerosus be cured?
At present, there is no cure for Lichen sclerosus, but treatment can relieve symptoms and help protect the skin from further damage.
It is estimated that around 60% of women will experience complete resolution of symptoms, while approximately 40% will continue to have symptoms that may come and go.
Treatment
- Steroid Ointment (see below)
- Emollients (moisturisers such as Zeroderm, Hydromol or Epimax) after washing and as required during the day.
- Soap Substitutes such as Dermol or QV for washing
Operations are not usually helpful because lichen sclerosus can come back in the skin that remains. Sometimes we may suggest surgery, if scarring or tightening of the skin makes it difficult to pass urine or causes problems during sex.
Are there any risks with Lichen sclerosus?
There is a small (around 3-5%) lifetime risk of developing a type of skin cancer on the vulva if you have lichen sclerosus.
Even though this risk is low, we recommend having a check-up at least once a year with your healthcare professional.
Additionally, self-examination allows you to monitor the condition yourself (see self-examination diagram).
You should always let your healthcare professional know if you have any ulcers, warty areas or bumps which are not healing with your steroid cream or are getting bigger.
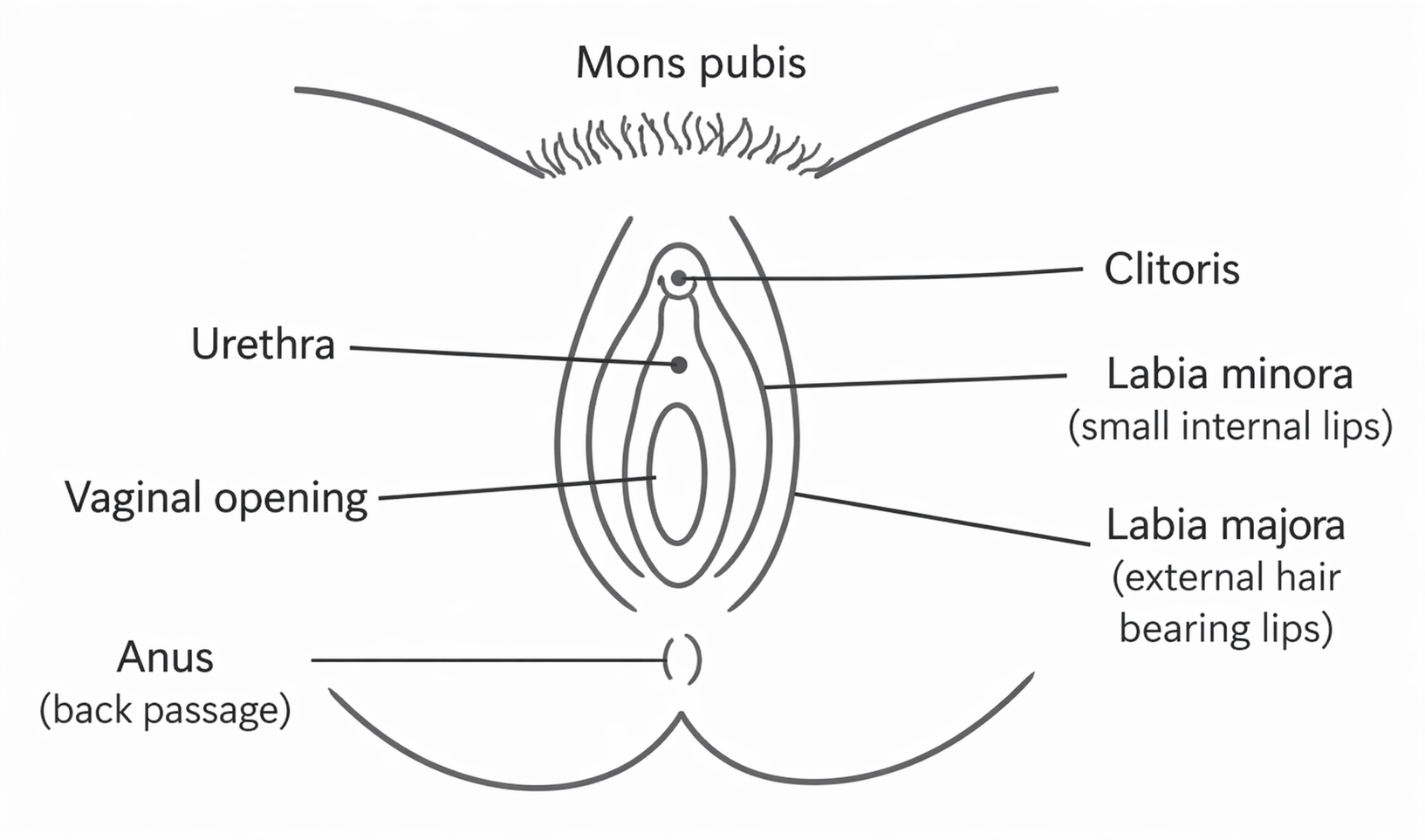
If you feel comfortable, it can help to check the area yourself using a mirror. The self‑examination diagram above shows the areas you can look at during your check.
For more support with self‑examination, you can ask your healthcare professional for help.
How to use the topical steroid (Clobetasol therapy)
Apply the cream or ointment sparingly (1/2 to 1 fingertip) to affected area:
- First month – apply to affected area every night
- Second month – apply to affected area on alternate nights
- Third month – apply to affected area twice a week
After the three‑month course, you may be advised to continue using it once a week long‑term. If you were told to stop but have a flare‑up, you can use the cream or ointment every night for two weeks to calm the symptoms and reduce itching. After this, try to lower how often you use it by following the steps above.
If your symptoms return when you stop, you may need to use the cream regularly for longer, slowly reducing to once or twice a week to maintain control. Long‑term use is safe as long as one 30g tube lasts at least three months.
If your symptoms do not improve when you restart daily steroids, we recommend seeing your healthcare professional, who can arrange a review with us.
A mild stinging sensation for a few minutes after applying the cream is normal. However, if the stinging lasts longer than 1–2 hours, you may be sensitive to the cream or ointment. If this happens, wash the area thoroughly and stop using the cream.
There are other creams available, and you should contact your healthcare professional for further advice.
Further information and support
For additional support and information about Lichen sclerosus, you may find the following organisation helpful: