Achilles tendinopathy is a common disorder that can cause pain, stiffness, swelling and weakness of the Achilles tendon.
Treatment protocols for Achilles tendinopathy almost always start with basic principles and we would encourage you to consider trying some self-help treatment in the first instance before making a referral to your local Physiotherapy department.
What is the achilles tendon?
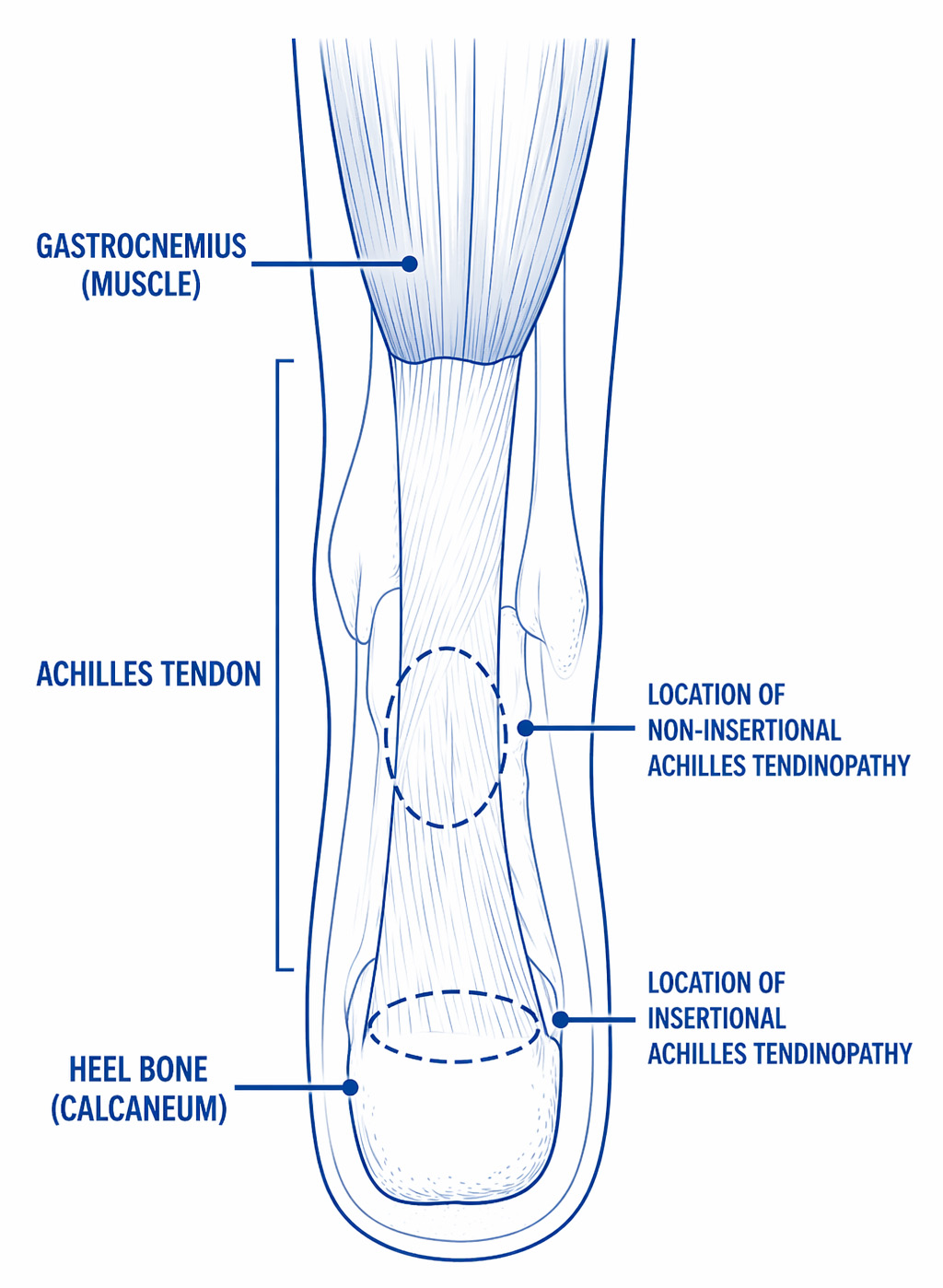
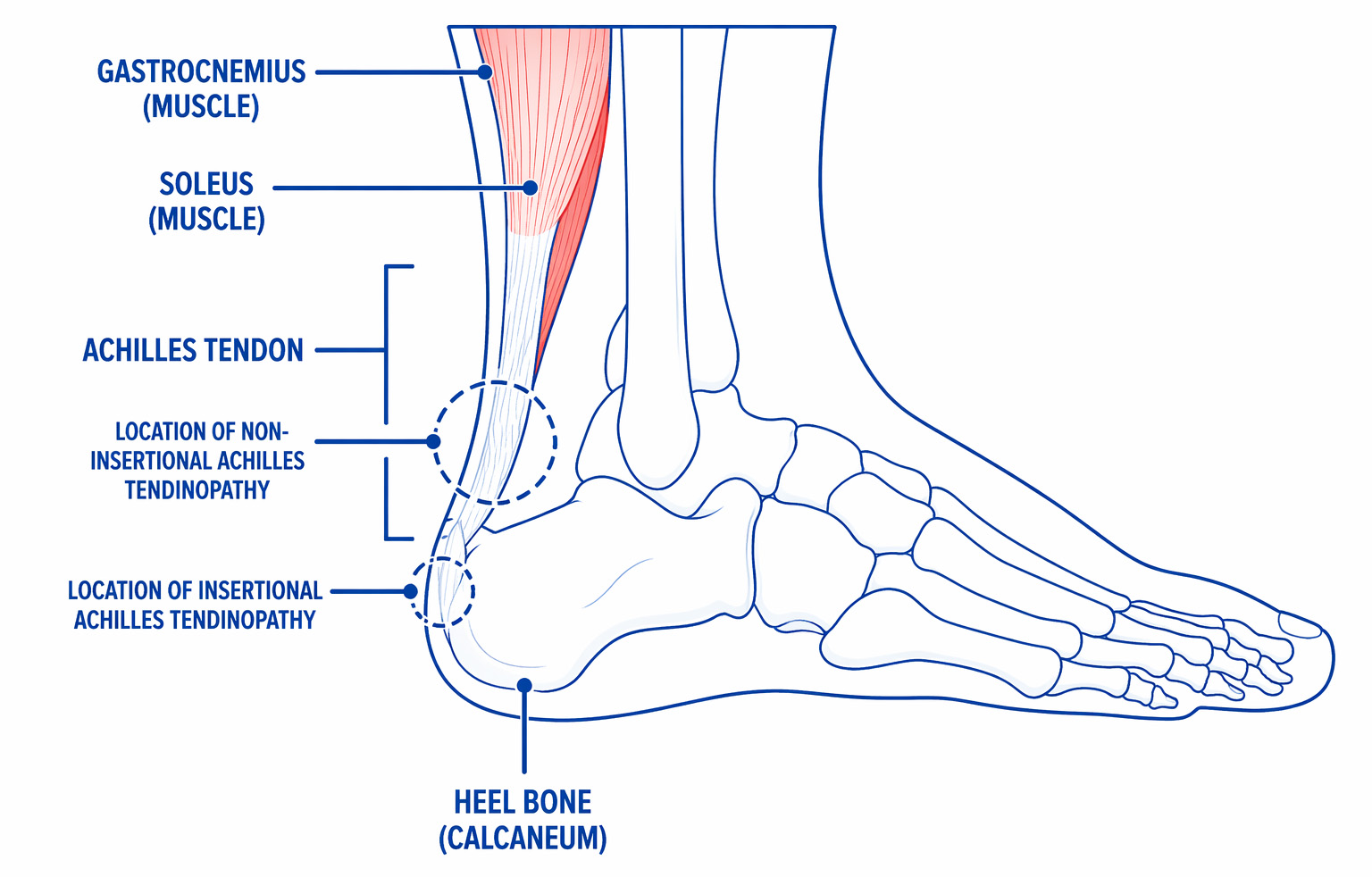
The Achilles tendon is both the longest and strongest tendon in the body. It connects both the gastrocnemius and soleus muscles, commonly known as calf muscles, onto the heel bone (calcaneum). It supports and absorbs the body’s weight while walking and running and can sometimes become over worked resulting in pain and discomfort. Achilles tendinopathy is usually categorized into either insertional or non-insertional pain. These require different treatments for a successful recovery.
What are the symptoms of achilles tendinopathy?
Non-insertional Achilles tendinopathy: This is the most common injury to the Achilles and affects the tendon around 2 to 6cm above where it attaches onto the back of the heel bone.
Insertional Achilles tendinopathy: The pain affects the tendon at the point where it attaches onto the back of the heel bone. This type of Achilles tendinopathy can be more complex.
Tendinopathy is usually diagnosed by taking a medical history and clinical findings and rarely needs further investigations or scans.
Classic signs and symptoms:
- Gradual onset of pain
- Pain and stiffness at the back of your heel during first steps when you get of bed or after a period of rest or inactivity.
- The tendon at the back of the ankle may be warm and tender to touch.
- The tendon may be swollen or thickened in appearance.
- There may be a clicking from the tendon when moving your ankle.
- Pain can differ from person to person. Some people will experience pain during exercise and others will notice that their symptoms become worse after exercise or weight bearing activities.
How common is it?
Achilles tendinopathy affects 150,000 people within the UK every year. It is most common in people between the ages of 30 and 50 years, however, it can occur at any age. It is more common in men than women and can affect both athletes and people who are not as active.
What causes it?
It is thought to be caused by repetitive stress and micro-trauma to the tendon as a result of a sudden increase in loading activities. A weakened or deconditioned tendon can be more easily injured.
The repetitive stress and microtrauma causes the normal ability to heal to slow which results in a painful Achilles tendon.
Other important contributing factors:
- Older age.
- Being overweight.
- Diabetes has been linked to increased risk of developing tendon problems.
- Inflammatory conditions such as rheumatoid arthritis, psoriatic arthritis etc.
- Weakness and/or tightness in the muscles within your feet or leg.
- Wearing unsupportive footwear such as shoes or sandals which have a low heel.
- Spending long periods of time standing or walking, especially with a sudden increase in these activities.
- Sudden increase in physical activity levels – for example, recently started running.
- Poor exercising/training technique and lack of recovery between activities.
- Prolonged use of oral corticosteroids and a certain family of antibiotics (Fluoroquinolones) can increase the risk of tendon problems.
- Smoking
What can help with achilles tendinopathy?
Helpful tips
The great news is that most people’s symptoms improve by following the recommended advice below, but it may take several months to get better.
If you have any of the contributing factors that can be changed it is important that you make the necessary changes to these. This will help your recovery.
Footwear
Wearing very flat shoes may aggravate your symptoms. A shoe that has a heel gradient of around 1 ½ inches (4cm) or inserting a 12mm rigid heel lift into the back of your shoe, under your heel, will help reduce some of the stress on the Achilles tendon. Always put a heel lift in both shoes even if only one tendon is painful.
Shoes that have flexible soles generally offer the foot less support and can increase the stress going through your foot and ankle. If your footwear has shoelaces make sure they are tied properly.
Avoid wearing hard, flat or unsupportive footwear.

Timescales/Prognosis
Most people with Achilles tendinopathy symptoms improve within 6 months of following the recommended advice, however, symptoms can take up to 1 year to improve in some people.
It is also normal to have periods of increased pain or flare ups during your recovery.
Pain activity ladder
By following the pain activity ladder you can identify activities that you would consider severely painful, moderately painful and mildly irritating and act to change your habits.
The pain scale, most often used in healthcare, measures pain from 0-10 (zero being no pain and 10 representing the worst pain you could imagine).
If you can identify the level of pain you are experiencing, you will find out if you are in the green, amber or red zone. The best way to move down to the green zone is by pacing and spacing your activity.
When you are completing your rehabilitation exercises it is often best to work within the green (and sometimes amber zones depending on what you deem is an acceptable level of pain) both during the exercises and within 48 hours of completing your exercises. If you find yourself in the red zone you are likely pushing yourself too hard and may flare up the pain.
Pacing and spacing
Pacing and spacing methods can help you manage your pain better.
Pacing is the term used for breaking down an activity or task. This can be done by taking regular breaks. Prioritising daily activities can also help. This can prevent “over stimulating” your pain system.
When completing challenging tasks or activities, it may be useful to set a “baseline”. This is the amount you can manage on a good or bad day without increasing your symptoms. Therefore, you can plan rests and set achievable goals.
If after following the above advice, your symptoms have not improved within 6 to 12 weeks, a referral to a physiotherapist may be beneficial. Speak to your GP about a referral.